|
KNEE AND SURGERY
|
||||
| English version of the website of Dr. J.E.Perraudin, french orthopaedic surgeon in Paris : www.docteurperraudin.com : the content is intended for general information only and does not replace the need for personal advice from a qualified health professional. Last updated Feb 12, 2017 | ||||
|
ANTERIOR CRUCIATE LIGAMENT
|
||||
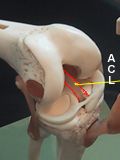 |
The anterior cruciate ligament (ACL) lies inside the knee joint. It crosses the other cruciate ligament called the posterior cruciate ligament (PCL). For more anatomic details, click here. The main function of the ACL is to prevent the tibia (shin bone) from rotating and subluxing under the femur (thigh bone) when the knee is twisted. |
|||
|
The anterior cruciate ligament provides stability when the knee is twisted between the foot being fixed onto the ground and the body twisting above it. This ligament is there-fore needed in sporting activities with "pivot": football, soccer, handball, gymnastics, ski...There are different theories as to why women are especially susceptible to ACL injury. If continuing these sports after a rupture of this ligament, it may lead to chronic instability that will make the knee prone to develop cartilage tears and early arthritis.
|
||||
| I THE INJURY
During the injury, the patient often hears a crack or a pop and the knee gives way. The swelling is frequent either quickly after the injury or the day after. Pain is often important when the injury occurs. If the patient tries to stand up, he may feel instable. II WHAT TO DO?
The orthopaedic surgeon will look for an associated injury of the lateral collateral ligament (lateral laxity) and quickly do a magnetic resonance imaging (MRI) if the clinical examination is difficult. No surgery in this acute phase, if there is no other injury to the knee (lateral collateral ligament, locking of the knee by a meniscal lesion) but icing, physiotherapy, drugs for pain relief and exercises to strengthen the muscle of the thigh (quadriceps) are to be continued. The magnetic resonance imaging (MRI) is a non-operating procedure that will confirm the diagnosis and assess the status of the ACL, menisci, cartilage and the other ligaments. (MORE) III WHO NEEDS RECONSTRUCTIVE SURGERY? Most patients are able to resume normal daily activities a few weeks after injury. The decision as to whether or not to operate on an ACL tear is dependent on several factors such as the age of the patient, the activity level of the patient (both recreational and occupational), the expectations of the patient, the ability and willingness of the patient to participate in post-operative rehabilitation, the degree of laxity of the joint, and any other associated injuries to the knee. It is necessary to consider surgery
In the other cases, if after six to eight weeks, despite the physiotherapy, the knee continues to give way when pivoting and if there is a laxity, it is appropriate to consider the reconstruction of the ligament. After surgery, most people can get close to a return to normal function if the procedure is without complications and the post-operative physiotherapy protocol is adhered to. Return to high level of competition may be difficult in high-demand sports. Some older patients do not need reconstruction if they do not participate in pivoting and cutting activities and if their knee is stable in daily life. It is proven by many studies that instability of the knee leads to early degenerative osteoarthritis. Docteur Jean Etienne Perraudin,
last updated 1 September 2012 |
||||
|
|
||||
|
|
||||